Mephedrone #
| Common Nomenclature | 4-MMC; 4-Methyl methcathinone |
| Street & Reference Names | Mcat; Mkat; Meow Meow; Drone; Bubbles; Plant Food; Bath Salts |
| Reference Dosage | ORAL Threshold 15mg+; Light 50mg+; Common 100mg+; Strong 150mg+ [Erowid] Light 50mg+; Common 100mg+; Strong 150mg+; Heavy 300mg+ [TripSit] FirstTime 100mg+; Average 150mg+; Strong 250mg [Drugs-Forum] INSUFFLATED Threshold 5mg+; Light 15mg+; Common 20mg+; Strong 75mg+ [Erowid] Light 15mg+; Common 20mg+; Strong 75mg+; Heavy 125mg+ [TripSit] |
| Anticipated: Onset / Duration | 30 Minutes / 4 Hours |
| Maximum Dose Experienced | 250mg *[See also 4.10 Supplementary Notes] |
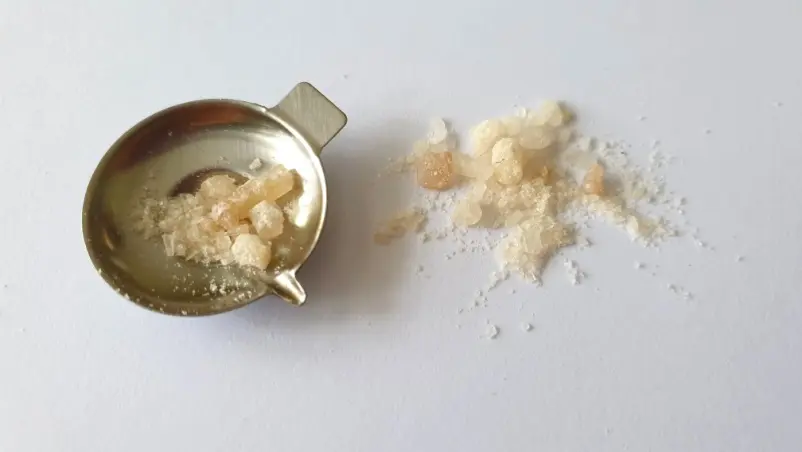
| Form | Crystal Powder |
| RoA | Oral, Insufflated |
| Source / Jurisdiction | Dealer / Overseas |

SUBJECTIVE EXPERIENCE #
First synthesised in 1929, mephedrone was rediscovered in 2003 (credited to Dr Zee). It became extremely popular from 2008, and indeed, at one point surveys suggested that it ranked alongside MDMA in terms of number of UK users.
This situation was greeted by a lengthy period of media hysteria, inclusive of flagrant exaggeration and outright propaganda, which even extended to deaths being falsely attributed to it. Inevitably it was soon classified in the UK (2010) and scheduled in the United States (2012).
Online, Erowid describes it as “a stimulant with empathogenic qualities”, whilst TripSit refers to it as “a short lived euphoric stimulant”. Drugs-forum.com offers this sensible suggestion
“Insufflating mephedrone can dramatically increase the urge to redose, therefore it is important users set out a maximum amount for the night and stick to it”.
This is advice which I will certainly heed.
I measure approx 150mg (156mg on the scale) and divide this into doses of 75mg, 25mg, 25mg and 25mg. I measure another 100mg for the scenario in which I wish to explore further. My absolute upper limit is therefore 250mg. I throw the rest away.
Insufflation is the most popular RoA. However, I elect to experiment initially via the oral route, and then subsequently snort a few lines. This approach does appear to be fairly common, particularly for lengthy sessions.
T+0:00 I wrap the 75mg in cigarette paper and bomb it with water. [2:50pm]
T+0:15 Other than the occasional shiver there has been no response thus far.
T+0:30 I perceive an increase in body temperature, and perhaps there is a minor heady feeling. These early signs, which indicate a slow-burning onset, are enough for me to hold off with the insufflation plan.
T+0:45 I now feel somewhat elevated and relaxed. There is a nice mild buzz to this: a certain high and uplift of mood. There are no rough edges or body load apparent so far, and this is certainly manageable. My pupils are half dilated and I am comfortably warm, apart from my hands, which are cool and clammy.
This is a nice level, although a little higher might be even better. I’ll see where this goes during the next 15 minutes and then take a further decision regarding the redosing.
T+0:55 I check my blood pressure for no reason other than curiosity. It is 175/89 with a BPM of 65. Whilst I brush this aside under the influence, I do realise that it is of concern.
T+1:00 An hour into the experience, I believe that the onset is complete. This is quite a happy level, and it isn’t too intense. I am feeling stimulation, euphoria and some empathogenic edge, which are all very pleasant.
Regarding horn, drive enhancement is certainly available, so I fully understand those users who articulate this aspect, although stim-dick seems to be a factor too (but not to the point of total dysfunctionality). The relatively short duration (compared to amphetamine) and thus the potential need for top-ups might also be issues to take on board here.
I am looking forward to the insufflation, as an increase in intensity would surely be enjoyable, but at the same time, online warnings that the snort is painful are fresh in my mind.
T+1:10 I bite the bullet and rail 25mg. This takes me to 100mg, 75mg of which was ingested orally. The snort wasn’t at all bad, and certainly nothing like as painful as some users suggested.
T+1:25 Surprisingly, there was no instant rush. Perhaps there has been a minor increase in intensity, but this seems to have crept up slowly rather than appearing suddenly.
I am as high as I have been, probably a little higher, but it has been a gentle incline throughout.
T+1:50 I am subjectively in a similar place to an hour ago, but with a greater sense of depth. My blood pressure is now 162/98 and my BPM is 69.
T+1:55 I snort the next 25mg. As this is proving to be extremely smooth and enjoyable, I also prepare the 100mg which I had put aside for a potential extension.
T+2:00 I insufflate the final 25mg of the primary batch. My total consumption is now 75mg oral and 75mg insufflated, which is well into common territory according to the harm reduction websites.
Within a couple of minutes this latest hit has elevated the high and noticeably increased its intensity. This is undoubtedly what is referred to as the rush. It has the same feel as earlier but is significantly headier in nature.
I am now flying high. It would appear that 150mg, at least of this particular sample, is my take-off threshold. This is consistent with a significant number of forum reports.
I would suggest that this is closer to MDMA than amphetamine. It is smoother and less physical than the latter, but not really as empathogenic as the former.
T+2:20 I am still at the new high, very warm (physically), and in a very contented and comfortable bubble.
It occurs to me that this would beat alcohol hands down if I was socialising. It has the feel of a drug to share with friends, although I am quite happy regardless.
T+2:30 I can understand how the desire to stay at this level leads to compulsive redosing, particularly as the duration is presented as short. Coming-down will be a drag. This is a danger of course, but it doesn’t feel like it whilst actually engaging.
T+2:40 There is some jaw tension now along with the urge to grind (resisted).
Although I am higher my pupils seem to be less dilated than earlier, which I find to be curious.
T+2:50 I insufflate the first 25mg of the 100mg reserve.
I feel that I now have a better understanding of this drug. There is indeed a rush, like an influx of euphoria, which is extremely rewarding. There is real temptation to chase it, again and again, as per the various reports and warnings.
It is very easy to see how users got through multiple grams of this over a weekend binge session when it was at the height of its popularity.
T+3:10 The second line of the 100mg reserve is fiendishly insufflated. The grand total has reached 200mg.
I am as high as the proverbial kite.
I check my pupils again: they are now more dilated than at any point previously.
T+4:20 The third line of the 100mg reserve is gleefully snorted, and 15 minutes later the final 25mg is hoovered.
T+5:20 I am still rolling, but not as intensely. This is slowly winding down.
T+5:40 I am gently returning to base. I feel no hangover or ill effects so far, and the urge to redose has dissipated. This is certainly one of the shortest acting chemicals of this class, which of course can be a positive attribute for some social occasions.
T+7:00 The show is almost completely over. There are some residue effects in play, including a little stimulation, but simultaneously I am becoming weary. My pupils are back to their normal size.
Following this adventure, I slept reasonably well, and there was no hangover in the morning. This was an entirely different aftermath to those I had endured with amphetamine and MDMA.
This was a very enjoyable experience, and one which confirmed the reputation of mephedrone for short term effect and the temptation to sustain the euphoric high via compulsive redosing. I suspect that this would be harder to resist in a more recreational environment, which in turn may have led to a less gentle landing. I would therefore re-emphasize the need to set a maximum dose in advance. It is probably also wise to stress the need for caution in terms of mixing this with other drugs, and of course, don’t skip the usual safety measures (Section 1.1).