MXP #
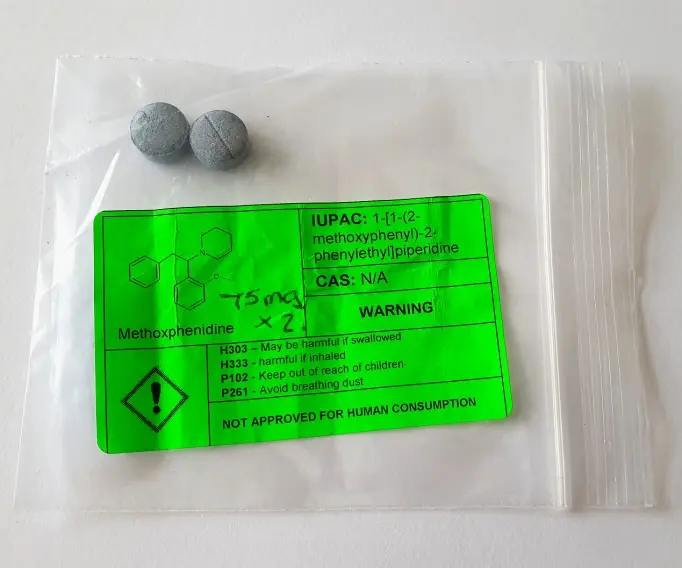
| Common Nomenclature | Methoxphenidine |
| Street & Reference Names | 2-MeO-Diphenidine |
| Reference Dosage | Threshold 15mg+; Light 40mg+; Common 75mg+; Strong 120mg+; Heavy 200mg+ [Erowid] Threshold 30mg+; Light 50mg+; Common 75mg+; Strong 120mg+; [TripSit] |
| Anticipated: Onset / Duration | 30 Minutes / 7 Hours |
| Maximum Dose Experienced | 50mg |
| Form | Pill |
| RoA | Oral |
| Source / Jurisdiction | Internet / UK |
| Personal Rating On Shulgin Scale | ++* |

SUBJECTIVE EXPERIENCE #
First referenced in a 1989 patent, MXP appeared on the recreational markets at the end of 2013, and became widely available during the following year.
My first experience with this chemical, a couple of years ago, was an early expedition into this field. I was well immersed, I enjoyed it, and I recorded it as a solid ++ on the Shulgin scale. However, other than its dissociative weirdness, and that I felt no ill effects, I recall very little about it.
Fortunately, I still have one old MXP pill of 75mg left in a desk-drawer. A decision is therefore required: what dose should I choose to re-sample with, given the threshold data above?
After the allergy test, there is perhaps 70mg remaining. As I recall Internet reports referring to seizures on high doses, there is an obvious need to proceed with more caution than usual. Further, the BlueLight forum warns of unpredictability and inconsistency, and suggests a starting dose of 50mg. I decide to heed this advice.
T+0:00 I break the pill into pieces, separate approximately 50mg, and bomb it down the hatch with water. [2:45pm]
I dispose of the rest to prevent redosing under the influence.
T+0:30 Already I am feeling a sedated headspace, and I dreamily drift off focus now and again. Whilst onset is commonly suggested to be 30-60 minutes, the odd report refers to two hours, which would put it on a par with my experiments with ephenidine. However, this has started to take effect much more quickly than anticipated.
T+0:45 I have now definitely entered the zone. Reality is a little weird, and a degree of anaesthesia is present. I am warm and comfortable, feeling a mellow headiness and physical insentience.
T+1:00 The headiness is pretty solid now, and quite pleasant. The physical feeling is interesting in that there are occasional tactile sensations amidst the overall numbing effect. Time is passing rather quickly. I am already enjoying it.
T+1:15 As weirdness would have it a David Bowie track rolls in the background with: “Please trip them gently, they don’t like to fall, Oh by jingo". I certainly feel that I am tripping gently at this stage, and floating.
T+1:30 The disconnection is now increasingly strong. I check my blood pressure: 163/91. It’s quite high but not alarming. My pulse is a normal 53bpm. I am not happy about the former, but in the interest of not increasing it further via stress, I choose to navigate my mind away from it rather than dwell upon it.
I take the experience into a more relaxing realm by playing some YouTube videos and reading.
T+1:45 Shock horror: a phone call! This takes me by surprise and I make the mistake of picking up the handset. The real world interjects and I desperately attempt to act like a normal human being. I engage a conversation to the best of my ability with the lady on the other end, but with difficulty. I believe that I am rational and lucid, but I am far from certain. I think the acronym I am looking for here is OMG.
With this trauma over, I try to put it behind me and settle back down into the experience.
T+2:00 I now feel that I have reached a plateau. The two hours have flown by. Although I am still a little haunted by thoughts of the mess I made of that phone call, I am in a fairly happy place.
I am a little chilly and my hands are cold, so there appears to be some vasoconstriction in play.
T+2:30 I feel a little more grounded, and have probably peaked, but I am still flying. There is a sense of wonder to everything as I float from one focus of concentration to another.
T+2:45 I am coming-down. Physically I still have cold and clammy hands, but mentally I am totally functional if I choose to be.
I can still ride the trip if I want to but step off it if I need to.
T+3:30 Time is still passing quickly. There is still some numbness and headiness but I am in a much gentler state of dissociation.
I find that I can choose a subject or topic, focus, and then fall into it for a period, before emerging back into self awareness.
I am now very much in control.
T+4:00 I seem to be winding down in the usual manner for a dissociative, but even at this level, the headspace, body analgesia, and tingles, continue to make this a gentle floating pleasure.
For the rest of the evening I drifted slowly but pleasantly down. Despite the bumps on the road I felt physically well and was able to navigate my mind into positive directions at will. The 50mg dose was clearly sufficient.
The night can best be described as comprising two deep sleeps of 3-4 hours each. The first began with chilliness and the need for an extra cover, and ended with a vivid nightmare. Theorising on the latter, I would speculate that, with the MXP still active at a low level, the intensification of focus upon subject matter took me deeper into the story of my dream than usual. This resulted in an extension of the dream beyond the point at which I would have normally woken, with greater immersion within it. I suspect that this phenomenon may also manifest across other dissociatives.
Notwithstanding the fact that generally I had a very good experience, research demonstrates that this is a chemical which clearly carries risks. Erowid, for example, reports that there have been several deaths associated with its use.
Dose moderation and appropriate caution is strongly advised.